“Cry ‘Havoc!’, and let slip the dogs of war.” – Shakespeare
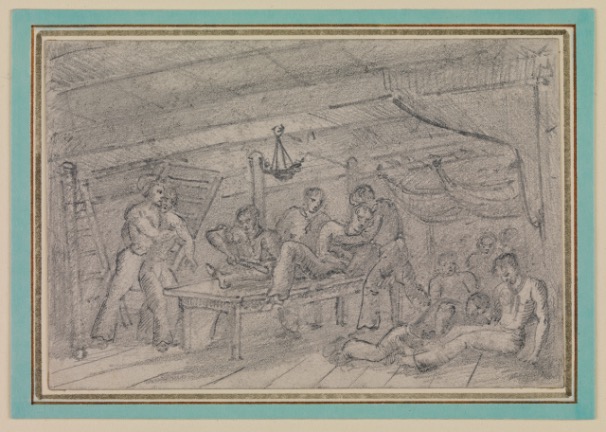
This rough sketch shows conditions in the cockpit of a naval vessel during battle. Wounded men are helped into the area and lie injured across the deck. On a table in the centre two sailors restrain a third who is having his leg amputated, without the benefit of anaesthetic. National Maritime Museum, Greenwich, London (ID: PAD8484).
Naval warfare in the age of sail was a ghastly business. As soon as the guns started roaring, the screaming of the wounded and the moaning of the dying would repeatably interrupt the deafening sound of the broadsides. As the battle developed and the smell of blood started mingling with the sharp stench of burning gunpowder, the unlucky stricken sailors were carried below-decks to be cared for by the surgeon. This article will succinctly discuss the perils of naval battles in the late 18th and early 19th century, as well as the efforts of the surgeon to help the victims of an engagement at sea.
The Dangers of Battle
When the opposing fleets were slowly moving towards each other, the hundreds of sailors in the cramped-up decks must have shared one sentiment: fear. The experienced crewmembers knew what they were in for: complete and utter chaos. As soon as the guns of the adversary started thundering and the cannon balls by way of whistling announced their imminent arrival, everyone braced themselves for the worst. It were actually not the balls themselves the British tars deeply feared, but the thousands of sharp wooden fragments sent through the ship upon their impact. As the smoke cleared and the destruction of the first endured broadside became visible, the stricken men made themselves be heard throughout the decks with their screams of agony. A crewmember in the Nelsonian navy was expected to be trained for such a situation. Before taking his maimed mate to the surgeon, he was to tighten a tourniquet above the wound – if possible – to avoid further blood loss. There was however a big difference in applying this instrument during the calm of a training session and during an actual battle when disarray was pressing him from all sides. After this quick procedure, the victim was taken to the surgeon belowdecks.
A wounded captain Henry Trollope of HMS Glatton during his action with a French squadron on the 16th of July 1796. Notice the tourniquet applied to his left leg where he received a musket ball. Print by Henry Singleton and James Daniell, 1797, NMM, Greenwich, London (ID: PAJ2247).
Meanwhile, on the upper deck other dangers loomed over the combatants. Not only did they have to watch out for incoming cannister, grape, chain and bar shots, but also enemy snipers, hidden in the masts, proved to be a serious menace. When brought within range, they cleared the decks of their opponents with their muskets, bringing hell from above. It was a bullet from a French sniper from the Redoutable which would mortally wound admiral Nelson during the Battle of Trafalgar. Finally, if a boarding was decided upon, it was the turn of the pistols, pikes, cutlasses and axes to prove their worth in battle. One could imagine the bloodiness of the ensuing fight with such weaponry.
Before the commencement of battle, the surgeon and his assistants had already prepared themselves for the incoming stream of wounded in the cockpit of the ship. The cockpit was situated on the orlop which is the lowest deck in a ship-of-the-line, just above the hold. This place was chosen for its relative safety from the guns of an adversary despite the horrible smell of putrid water from the nearby bilges. Besides his assistant-surgeons the surgeon was usually assisted in this operating area by the other non-combatants such as the clerk, chaplain, purser and stewards. Since the cockpit was very dark, one of the first things to be taken care of was proper lighting with candles and lanterns. Then the surgeon and his assistants would usually shove together the chests of the midshipmen to form some sort of waiting area where the wounded could be seated. For those who could not be seated, canvas and bedding were laid down on the floor. Then tubs were filled with water in which the doctor could wash his hands and surgical instruments and empty buckets were provided in which to put amputated limbs. A portable stove was to be ignited to heat up water for the amputation-saws and knives. There was in fact nothing as agonizing as the feeling of ice-cold steel making its way through your flesh and bone. Bottles of spirits were also close at hand for refreshening after an operation. It is however a myth that alcohol was used to sedate the patients. The surgeons were back then already aware of liquor’s blood thinning effect which slowed down blood clotting. To alleviate the pain the ship’s surgeons mostly used the opiate, laudanum. In order to clean the wounds, the navy was to provide linen, but this was rarely available. Often it was deemed too expensive and replaced with sponges. During battle, their amount could prove to be insufficient very quickly, thus forcing the surgeons to re-use the dirty ones. This ironically and sadly led to death by blood-poisoning of even the most lightly wounded men.
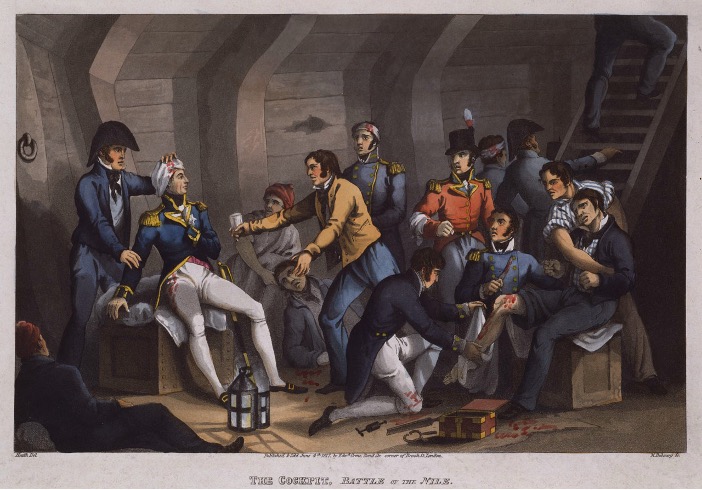
Print showing the cockpit of HMS Vanguard during the Battle of the Nile (1 Augustus 1798) with a wounded Nelson to the left. To the right a sailor is preparing himself for the amputation of his leg. Print by M. Dubourg and William Heath, 4 June 1817, National Maritime Museum, Greenwich, London (ID: PAD5574).
As soon as the first enemy broadside had made its way through the ship, the first wave of wounded arrived whose number in a heated action could amount up to twenty. From this point on, everything happened very fast. One surgeon on the ship meant that only one man at a time could be looked after. Everyone was treated equally, regardless of rank and seriousness of the wound: you had to wait your turn. The downside of this method was that some had already bled to death before the doctor got to them. Upon arrival of a new patient the surgeon had to give him a quick glance to assess the wound. He then had to make the hard decision whether the man was beyond saving or not: in these circumstances one could not waste its time on a sailor with a very low likelihood of survival. The only thing that could be offered to these doomed tars were Christian consolation and compassion from the chaplain.
As illustrated above, the cause and thus the character of an injury could be various. Most common were lacerations of the flesh and fractures of the bone incurred by sharp wooden fragments, flying about through the hull with great velocity after the fiery arrival of an enemy cannonball. The surgeon had to extract these splinters as quickly as possible with probes after having removed the skin with a fleam. If not, the stricken sailor was likely to die from a tetanus infection. When a tar was hit by missile projectiles from cannon, musket or pistol fire, the surgeon would make use of his extractors to remove the remaining pieces. The best he could hope for in these cases was that the bone remained intact. Shattered bones proved to be the most challenging injuries to operate and the most difficult for the victim to survive. The surgeon also had to be prepared to treat men with burns. Despite the precautions taken, there still was a considerable risk that the cartridges, stowed away in wooden cases, would ignite during the mayhem of battle. Another ever-present danger for the gun crews were scorches caused by the flashes of the burning gunpowder at the touch holes of the cannons. In Nelson’s time the navy in fact used slow-match artillery pieces which did not sufficiently protect the sailor from the flaring black powder. Later, however, the introduction of flint-operated gunlocks dismissed this peril and injuries from operating guns almost completely disappeared. Finally, in case of a boarding, men would arrive at the cockpit with penetration wounds from hand-to-hand combat. The seriousness of the injury was based upon its proximity to the vital organs. The most serious of these wounds would have caused internal bleeding. When this was the case, the surgeon often first performed a bloodletting to decrease the blood pressure which would in turn enhance the clotting process. His main objective then was to halt the haemorrhaging by suture of pressure bandaging.
When a limb was too badly maimed, the surgeon could still resort to the extreme measure of amputation. According to the rules, this was to be the final option, but the mayhem of the circumstances could easily lead to a lack of sound judgement and unnecessary irreversible mutilation. The reputation of the surgeon during the Revolutionary and Napoleonic Wars was indeed very poor. In any case, when amputation was decided upon, the operation had to be carried out as quickly as possible. The procedure should not last any longer than twenty minutes in order to avoid too much blood-loss. Most surgeons were trained to complete the operation in a staggering two minutes! Even then, the survival rate was only about fifty percent. First, the patient was anaesthetized with laudanum and a tourniquet was fastened above the wound to numb the limb as much as possible. The sailor was also given a patch of leather to bite on during the surgery. The surgeon then made a circular cut just below the place of amputation. He peeled back the skin upwards. The whole point of this was to have some skin in reserve to seal off the amputated arm or leg afterwards. Then the amputation itself could begin. The surgeon would cut through the flesh with a knife and then the bone with his saw. He’d then close the blood vessels temporarily with forceps and afterwards permanently with ligatures. Then the earlier mentioned flap of skin was wound over the stump and stitched together. The whole was finally disinfected with turpentine.
The treating of the stricken sailors could prove to be an exhausting job for a naval surgeon. The surgeon of HMS Ardent, Robert Young, for example had to work around the clock on the 90 casualties of his ship during the Battle of Camperdown (11October 1797) until 4:00 AM despite the guns being silent since 3:15 PM.
Example of an amputation knife: Surgical knife belonging to Dr David Livingstone (1813-1873). Liston double-edged amputation knife, with a hard wood handle with a textured grip and a steel blade. National Maritime Museum, Greenwich, London (ID: ZBA6707).
In short, serving as a sailor in the Royal Navy was a risky business in the age of Nelson. Broadsides, musket fire and hand-to-hand-combat took their toll. The overall performance of surgeons during battle could vary significantly. Some were excellently trained. A great part however lacked sufficient education which could lead to unnecessary loss of life. This prompted the much-revered naval physicians Gilbert Blane, Thomas Trotter and John Harness to advocate serious health reforms during the Revolutionary and Napoleonic Wars. These attempts would prove fruitful and steadily into the 19th century the quality of Britain’s naval surgeons would improve. Furthermore, the transformation of the Royal Navy from a wooden wall into a wall of steel completely changed the environment of the British tars as well as the types of wounds they could suffer. They dreaded splinter-injuries became a thing of the past and this to much relief of the crew members.





Leave a comment